Prevention of undernutrition in humanitarian contexts
In humanitarian and food security crises, preventing undernutrition is critical to saving lives, protecting human dignity and fostering long–term recovery and resilience.1 The case for the prevention of undernutrition is increasingly recognised in several areas including:
Life–saving impact that helps to ensure immediate survival by reducing the risk of death from starvation, disease, or infections exacerbated by undernutrition.
Prevention of long–term developmental damage such as stunted growth and poor cognitive development in children and the damaging generational impacts on infants and young children of undernutrition in women and girls.
Preservation of health systems through reducing the burden of malnutrition and disease on services
Promotion of resilience and recovery enabling individuals and communities to participate in rebuilding efforts, economic activities and social recovery.
Prevention of conflict and social unrest through reducing the tensions caused by food insecurity and undernutrition.
Ethical and human rights obligations that supports the humanitarian principles of human dignity and protection through providing safe access to adequate food and nutrition, supporting psychosocial well–being and child/ women–centred action and ensuring that undernutrition does not disproportionately affect those who are least able to cope with its effects.
The importance of investing in actions to prevent undernutrition in humanitarian contexts is now gaining traction within national Governments and all leading humanitarian agencies. Whilst this is most recently shown by its prominence in the new WHO (2023) guidelines on the prevention and management of wasting and nutritional oedema,2 there remains a gap in available recommendations and detailed guidance for the design and delivery of any prevention component.
The importance of investing in actions to prevent undernutrition in humanitarian contexts is now gaining traction within national Governments and all leading humanitarian agencies.
Aims and objectives of this tool
The objective of this decision tool and resource package is to support governments, donors and coordinating and implementing agencies working in food insecure humanitarian contexts to design and deliver a response that will support the effective prevention of undernutrition among pregnant and breastfeeding women and adolescent girls (PBWGs) and children under five years.
This tool aims to support the design of a complete multisectoral response delivered (most commonly) by multiple actors to address the most common and immediate drivers of undernutrition across diverse humanitarian settings. It is relevant for agencies involved in the design and/or coordination of a holistic multisectoral response as well as agencies covering one or two components. It will help to ensure prioritisation of key actions within a collective response, as well as giving options on interventions and the considerations that are important.
The tool does not aim to cover the detail of programme design which can be found in the large body of existing technical guidance and learning that are linked in the resource pages of this tool.
The tool is process–oriented: it covers the importance of understanding the main causes of undernutrition in a specific context as a first step; design of a holistic multisectoral response corresponding to this analysis and the oversight and coordination needed for implementing actors. The range of evidence–based nutrition–specific and nutrition–sensitive interventions that can be selected according to the context and target group is also presented with some guidance on the process of response design to ensure that the basic needs of those most vulnerable to undernutrition ie, PBWGs and children under five, are met.
The objective of this decision tool and resource package is to support governments, donors and coordinating and implementing agencies working in food insecure humanitarian contexts to design and deliver a response that will support the effective prevention of undernutrition among PBWGs and children under five years.
The rationale for a multisectoral approach to preventing undernutrition
Since the early 1990s, there has been a significant evolution in the understanding of nutritional status as an outcome of multiple, interacting determinants across a variety of sectors and at different levels.
The UNICEF Conceptual Framework of the causes of malnutrition,3 first developed in 1990, articulated the drivers operating at different levels:
Basic drivers reflect political and structural challenges, including social, economic, environmental and political leading to lack of or unequal distribution of capital.
Underlying drivers include factors at household level such as food insecurity, inadequate care and feeding practices, limited access to healthcare services and to a hygienic environment (including safe drinking water and sanitation services).
Immediate drivers are inadequate food intake and disease, as a result of the impact of basic and underlying drivers at individual level.
Since then, there has been an increasing body of evidence linked to the different factors that influence nutritional outcomes. 4,5,6,7,8 The development of the Lancet framework for action to achieve optimum foetal and child nutrition and development,9 built on the UNICEF Conceptual Framework and describes the pathways to improved nutrition at different levels and across different sectors. It proposes a range of possible nutrition–related interventions across sectors including health, agriculture and food systems, water, sanitation and hygiene (WASH), social protection and education, as well as cross–cutting actions (eg, advocacy and women’s empowerment), which combine to form a multisectoral and holistic approach to improving nutrition outcomes.
Model of a multisectoral approach for the prevention of undernutrition in humanitarian contexts
We have adapted the Lancet framework (Figure 1 below) to focus on the multisectoral intervention areas that are needed for prevention of undernutrition in humanitarian contexts. Adaptations include the addition and/or specification of intervention areas that are particularly relevant for humanitarian response and the removal of those that, whilst important for development programming, may be less relevant for humanitarian settings.10 This model supports the first step in thinking about which sectors need to be involved and how they contribute to the joint aim of preventing undernutrition. More detail linked to delivery and design of many of these actions are provided below under the decision tool.
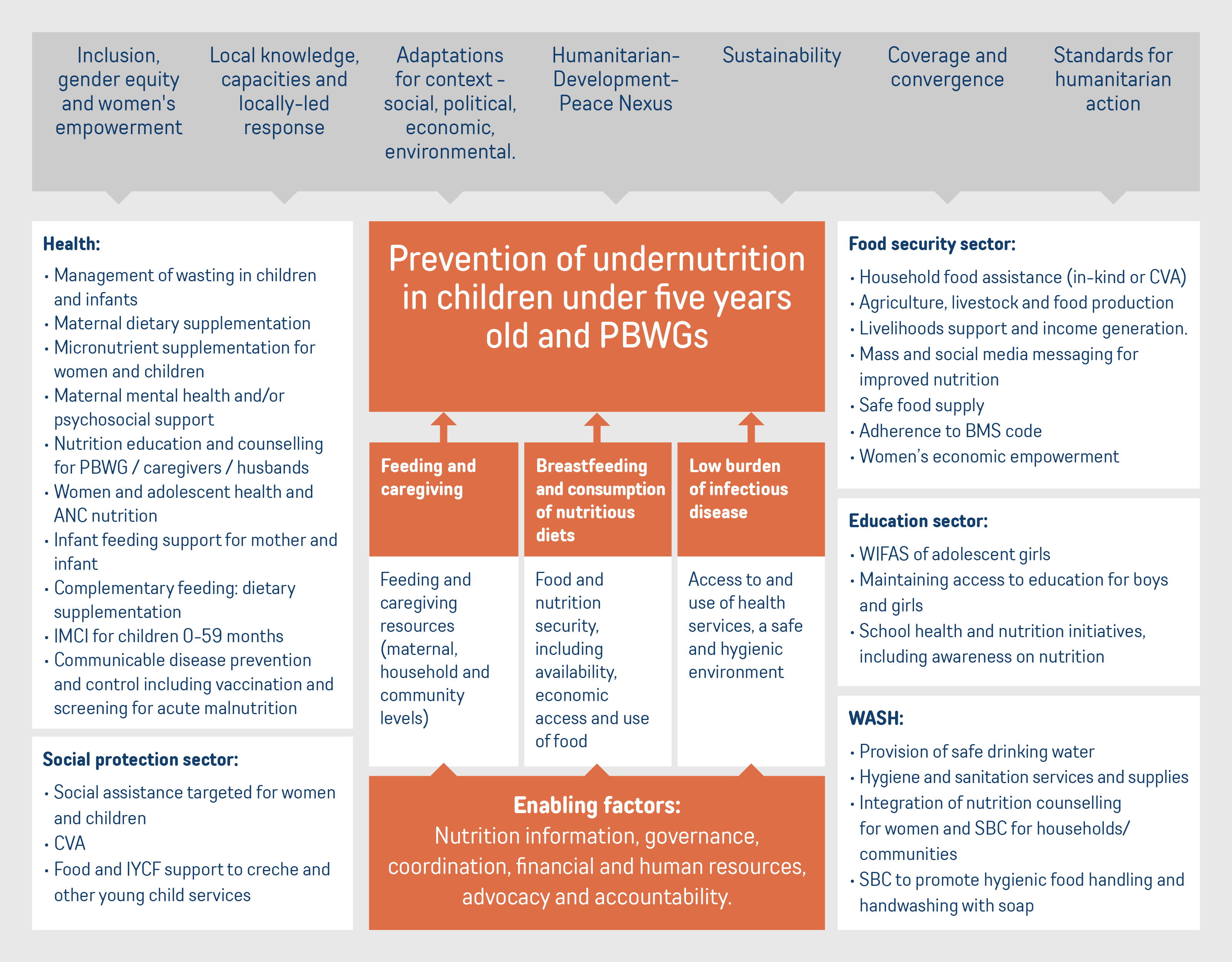
Figure 1: Conceptual model of a multisectoral approach to the prevention of undernutrition in humanitarian contexts, adapted from the Lancet framework
We have summarised the evidence for a range of the key intervention areas detailed in Figure 1.
It is now well–accepted that in contexts where there is a high burden of undernutrition or where nutritional status is at risk (eg, due to an emergency or acute food insecurity), a multisectoral and convergent response is required to deliver a set of interventions to those most vulnerable to undernutrition, based on a context–specific understanding of the main drivers.
Mapping the evidence across sectors and interventions
The Evidence Review,11 that formed the first step in the development of this decision tool, concluded that a combination of interventions is more effective at preventing undernutrition than separately implemented interventions. The available evidence shows this to be particularly true of the combination of cash or voucher assistance, food supplementation and/or agricultural/food production and of the addition of nutrition–related SBC to any of these interventions. There is growing evidence that demonstrates the importance of addressing women’s empowerment – including support to women’s agency, engagement and leadership – as part of multisectoral interventions to improve nutrition impacts.
Concurrent provision of these combined interventions during critical periods such as preconception, pregnancy and early childhood is recommended. Evidence in some intervention areas is less strong than in others, and more evidence in these areas would help to strengthen understanding of the most effective and cost–effective combinations of interventions needed to prevent undernutrition in different contexts.
References
1 For the purpose of this tool the term undernutrition includes wasting, stunting and micronutrient deficiencies all of which frequently occur at high levels in the same populations affected by food insecurity and crisis and which commonly share the same risk factors. A multisectoral response that aims to address all these forms of undernutrition simultaneously where they occur, makes optimal use of resources and can improve the cost effectiveness of programming. (Thurstans, S., Sessions, N., Dolan, C., et al. (2021). The relationship between wasting and stunting in young children: A systematic review. Maternal & Child Nutrition, 18:e13246. https://doi.org/10.1111/mcn.13246 and Emergency Nutrition Network. The need to consider Wasting and Stunting together Talking Points for a Donor Audience. Sept, 2024)
2 WHO (2023) WHO guideline on the prevention and management of wasting and nutritional oedema (acute malnutrition) in infants and children under five years. Geneva: World Health Organization. Available at: https://app.magicapp.org/#/guideline/ noPQkE
3 UNICEF, 1990 and 1992, A UNICEF policy review: Strategy for improved nutrition of children and women in developing countries. UNICEF, New York
4 Black, R. E. , Alderman, H. , Bhutta, Z. A. , Gillespie, S. , Haddad, L. , Horton, S. , Lartey, A. , Mannar, V. , Ruel, M. , Victora, C. G. , Walker, S. P. , & Webb, P. (2013). Maternal and child nutrition: Building momentum for impact. The Lancet, 382(9890), 372–375. 10.1016/S0140-6736(13)60988-5
5 Black, R. E. , Allen, L. H. , Bhutta, Z. A. , Caulfield, L. E. , de Onis, M. , Ezzati, M. , Mathers, C. , Rivera, J. , & Maternal and Child Undernutrition Study Group . (2008). Maternal and child undernutrition: global and regional exposures and health consequences. Lancet, 371(9608), 243–260. 10.1016/S0140-6736(07)61690-0
6 Shekar, M. , Kakietek, J. , Dayton Eberwein, J. , & Walters, D. (2017). An investment framework for nutrition: Reaching the global targets for stunting, anemia, breastfeeding, and wasting. The World Bank.
7 Victora, C. G. , Christian, P. , Vidaletti, L. P. , Gatica‐Dominguez, G. , Menon, P. , & Black, R. E. (2021). Revisiting maternal and child undernutrition in low‐income and middle‐income countries: variable progress towards an unfinished agenda. The Lancet, 397, 1388–1399. 10.1016/S0140-6736(21)00394-9
8 Keats, E.C. et al. (2021) ‘Effective interventions to address maternal and child malnutrition: an update of the evidence’, The Lancet. Child & Adolescent Health, 5(5), pp. 367–384. Available at: https://doi.org/10.1016/S2352-4642(20)30274-1
9 Black, R.E. et al. (2013) ‘Maternal and child undernutrition and overweight in low-income and middle-income countries’, The Lancet, 382(9890), pp. 427–451. Available at: https://doi.org/10.1016/S0140-6736(13)60937-X
10 Specific intervention areas that were removed include biofortification and agronomic fortification; Policies to reduce prices or increase access to nutritious foods and diverse diets.
11 Sadler K, Walters T, Brown R, Cherotich L, Abi Akar R. (2024) ‘Multisectoral prevention of undernutrition for food insecure contexts: An evidence synthesis’. Elrha: London. Elrha_Prevention-of-Undernutrition_Evidence-Synthesis_Final-082025.pdf